The TOPS™ System is a lumbar facet joint replacement implant which stabilizes the spine without a rigid fusion. The TOPS is implanted at the diseased level (typically L4-L5, L3-L4, or L2-L3) following decompression surgery to alleviate pain stemming from spinal stenosis and degenerative spondylolisthesis. Spinal stenosis is a narrowing of the spinal canal, which causes a pinching of the spinal cord and nerve roots that extend from the spine to the legs. Degenerative spondylolisthesis refers to an abnormal slip of one spinal vertebra in relation to another that causes pain in the lower back and legs. The TOPS™ System is indicated for spinal stenosis and spondylolisthesis from L2 to L5.
TOPS / Nexux Prosthesis
Lumbar Facet Joint Replacement
Nexux
30% smaller than original TOPS prosthesis

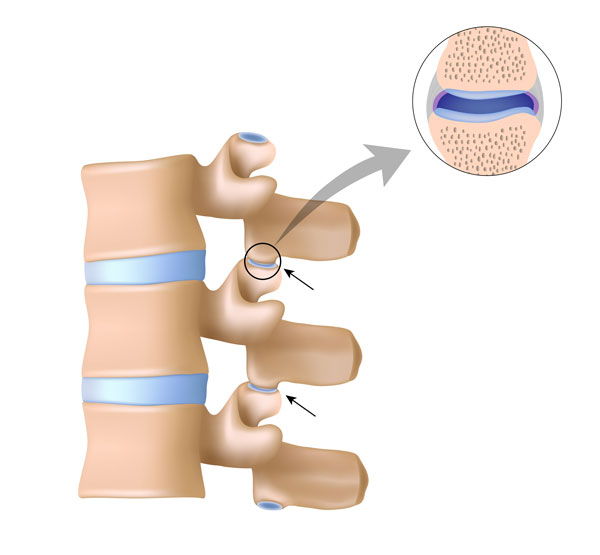
What is a facet joint?
Every level of your spine contains two facet joints. Each pair of facet joints guides and limits movement of the spinal motion segment. In the lumbar spine, for example, the facet joints function to protect the motion segment from anterior shear forces, excessive rotation and flexion. These functions can become damaged and painful by degeneration, dislocation, fracture, injury, osteoarthritis, and instability from trauma. Cavitation of the synovial fluid within the facet joints is responsible for the popping sound (crepitus) associated with manual spinal manipulation, commonly referred to as “cracking the back.”
TOPS Facet Joint Replacement
The TOPS™ system completely replaces the damaged facet joints to bring back stability and proper motion of the spinal segment. Our surgeons have extensive experience with the TOPS™ and Nexux facet joint replacement systems. They are involved in the ongoing development of these systems and they teach this surgical procedure to other surgeons around the world. The TOPS™ System has been proven more effective than a spinal fusion from long term 7-year follow up studies. This is a promising area of development in modern spine surgery.
The TOPS™ System provides three major benefits for the treatment of spinal stenosis, spondylolisthesis and other diseases of the facet joint. First, the procedure stabilizes the lumbar spine and reestablishes a controlled range of movement. Second, patients regain their ability to bend, flex, walk, and enjoy the normal activities of life. Third, and most importantly, patients experience immediate and sustained pain relief. Clinical studies conducted since 2005 show the TOPS™ System alleviates persistent leg and low back pain for patients with moderate to severe spinal stenosis with or without spondylolisthesis (a slipped disc) and facet arthrosis (bone spurs).

Other Procedures at ONZ
Not everyone is a good candidate for facet joint replacement surgery and sometimes a different procedure is the best way go. Our experienced surgeons have many tools in their toolbox to address many different types of spinal conditions. Dr. Bierstedt, Dr. Illerhaus, and Dr. Ostermann are unbiased and will recommend the best treatment for your unique case.
Artificial Disc Replacement (ADR), sometimes referred to as Total Disc Replacement (TDR), is a motion preserving spine surgery where the original flesh discs are replaced with an artificial disc. ADR was pioneered in Germany in the 1980s and since then, we’ve learned what works, what doesn’t, and have made great progress in evolving the technology. Today, the discs that we use provide elastic return just like a real human disc. They also provide all 6 degrees of motion including shock absorption (cushion) as well as controlled flexion, extension, and rotation as opposed to older disc designs that had uncontrolled or too much movement. The 3rd generation discs that we’re using today are better, more reliable, and designed to last for many decades.

Some patients who want to avoid a fusion on multiple levels in their lumbar or cervical spine might be a good candidate for a hybrid procedure. With a hybrid, the patient will have a combination of ADR (artificial disc replacement) at one or more levels and a fusion at one or more levels. This hybrid solution allows the patient to still maintain some motion while decreasing the risks for adjacent level disease (sometimes called adjacent segment disease) which is common with stand alone fusions.
The Joimax TESSYS®method uses the lateral transforaminal endoscopic approach, which is, in general, a “gentle surgery.” TESSYS® can be used for all kinds of deherniation or decompression of the lumbar spine (including L5/S1). The intervertebral foramen is used for safe access to the spinal canal. In order to avoid irritation of the nerves in the foramen, the caudal part of the intervertebral foramen is widened millimeter by millimeter using special reamers. Especially, if due to location of the pathology or the age of the patient the foramen is narrow. In that case bone material has to be removed. Using special endoscopes with a working channel, herniated disc material can be removed with forceps.
An anterior lumbar fusion is performed from the front side (through the abdomen) instead of the back. The approach is the same as with an artificial disc replacement (ADR), but instead of replacing the flesh disc with a motion preserving prosthesis, the disc is replaced with a rigid spacer or cage that is designed to fuse two vertebrae together.
Why an ALIF?
Our goal is to preserve motion at the segment when possible, but depending on the spinal condition, an anterior fusion might be the best solution for the patient. Our ultimate goal is to provide spinal stability and relieve the patient from as much pain as possible, which the ALIF allows us to accomplish.

A posterior lumbar interbody fusion is performed from the back side of the patient. As opposed to an ADR where the goal is to preserve motion, the goal for a PLIF (and ALIF) is the opposite – to stop motion. With the posterior fusion, the flesh disc is replaced with a rigid spacer or cage that is designed to fuse two vertebrae together. In addition to the spacer, rods and screws are added to correct and rebuild spinal alignment and provide the needed stability.
Why a PLIF?
Our goal is to preserve motion at the segment when possible, but depending on the spinal condition, a posterior fusion might be the best solution for the patient. Our ultimate goal is to provide spinal stability and relieve the patient from as much pain as possible, which the PLIF allows us to accomplish.

When faced with a posterior interbody fusion (PLIF), sometimes it’s possible to use a screw with a hinged joint that provides the necessary dorsal dynamic stabilization but while also preserving some mobility within the segment. These screws feature a rotation-stable joint design and Bonit coating which helps accelerate osseointegration and healing.
Why Flexible Stabilization?
Our goal is to preserve motion at the segment when possible and these flexible screws help in preserving some motion when faced with a PLIF.
Screw with Hinged Joint

Begin the Evaluation Process
Take the first step towards getting your life back and contact us today.
Copyright ©2024 all rights reserved
Visit www.onz-online.de for our full spectrum of ONZ orthopedics and neurosurgery